This article builds on my recent piece, Audit the Mix: Why Health Systems Must Reevaluate Their IT Staffing Strategy, where I argued, inspired by Jim Collins’ principle in Good to Great, that today’s imperative is not just to get the right people on the bus, but to ask: do we need more than one vehicle? Health IT leaders must now consider not only who is on the team, but also the structure and purpose of the vehicles driving delivery.
In this follow-up, I lay out the behavioral, cultural, and structural traps that get in the way of smart staffing and resourcing decisions in health IT. These are the blind spots that prevent leaders from building the right mix of FTEs, contractors, and external partners—even when the rationale is obvious. When they’re left unchecked, the outcome is predictable: bloated teams, misaligned capacity, and wasted resources. The table below summarizes the most common traps I see—and why they need to be addressed head-on.
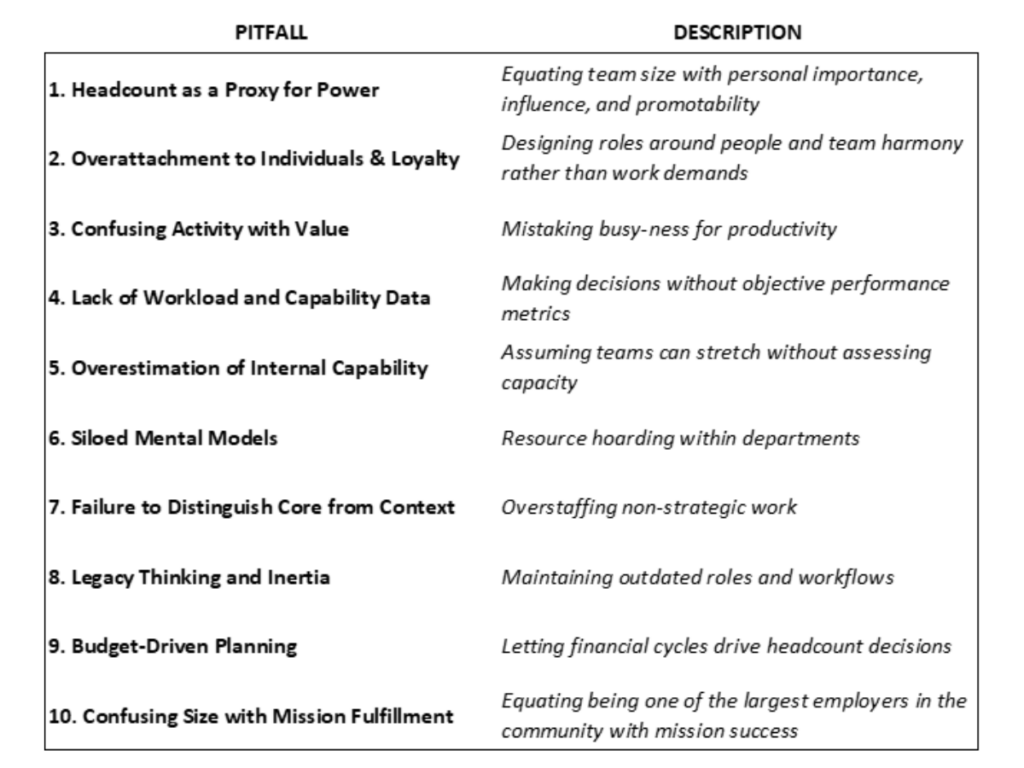
Below, I unpack these pitfalls in more detail and suggest how IT leaders can avoid them.
1. Headcount as a Proxy for Power
IT leaders in many health systems often equate team size with influence, especially in environments where budget, authority, and promotion opportunities are tied to organizational charts. This can lead to resistance to outsourcing, implementing automation tools, or consolidating services into shared models. But clinging to headcount as a measure of value prevents leaders from aligning their teams with the agile, scalable needs of the health systems they serve. This mindset conflicts with a dynamic labor strategy that recognizes not all work merits in-house FTE investment. Leadership value should be measured in terms of impact, not span of control. In a blended labor model, effectiveness often means fewer, but better-aligned internal roles.
2. Overattachment to Individuals and Loyalty
Health systems often foster close-knit, long-tenured IT teams. While this culture creates loyalty, it can lead to decision paralysis when it comes to reskilling, reassigning, or exiting team members whose roles no longer align with strategic needs. Designing your team around legacy individuals rather than current work requirements undermines adaptability. Being people-first does not mean preserving roles that no longer serve strategic outcomes. True leadership requires reallocating talent in service of the mission, not entrenching teams in outdated models. Redeployment is often the more humane and strategically aligned path than indefinite role protection.
3. Confusing Activity with Value
In busy hospital environments, high ticket volumes or long hours can give the impression that more staff are needed. But without analyzing whether the work is low-value, duplicated, or suitable for automation, leaders risk deploying additional staff at challenges better solved by process redesign or technology. Especially now, with CIOs under pressure to justify every dollar, it’s critical to focus on outcomes, not activity.
4. Lack of Workload and Capability Data
Many health systems still lack real-time visibility into how work is distributed across their IT teams. Without data on actual workloads, skill gaps, or cycle times, staffing becomes guesswork. A quarterly staffing audit—reviewing role utilization, partner SLA performance, and cost-to-value ratios—is essential to shift from gut feel to fact-based resourcing. In an era of operational margin compression, this kind of audit is not optional—it’s foundational.
5. Overestimation of Internal Capability
Taking on a community connect provider, enterprise data warehouse, or digital front door initiative with existing staff who are already stretched thin may be a recipe for failure. Leaders must be honest about internal bandwidth and bring in partners or temporary resources where needed. Underestimating effort and overloading staff leads to burnout, turnover, and stalled projects. Flexible capacity isn’t weakness—it’s how you protect core talent from unsustainable stretch.
6. Siloed Mental Models
Health systems are often structured around service lines or facilities, and IT can mirror this fragmentation. Leaders may duplicate roles like analysts or support techs across departments rather than leveraging shared services. Shared technical analysts or centralized app support functions can offer efficiency without sacrificing responsiveness. In an era where scalability and interoperability are vital, this siloed thinking is not just inefficient—it’s risky.
7. Failure to Distinguish Core from Context
Health IT leaders must distinguish between core work (e.g., cybersecurity, data governance, innovation strategy) and context work (e.g., password resets, device deployment, application support). The former deserves in-house investment. The latter should be streamlined, automated, or outsourced. Context work is ideal for outsourcing partners. This clarity frees internal teams to focus on what only insiders can do. This distinction frees internal teams to focus on what only they can deliver. It also guides smarter decisions on staffing, skill development, succession planning, and technology investment.
8. Legacy Thinking and Inertia
Healthcare IT is notorious for maintaining legacy systems and structures due to regulatory complexity and provider preferences. However, holding onto obsolete roles or redundant processes under the guise of “we’ve always done it this way” is especially dangerous now. With pressure to do more with less, IT leaders must be willing to reimagine roles considering cloud migrations, outsourcing and co-sourcing options, automation, and emerging digital health platforms. This inertia often masquerades as risk avoidance—but the real risk lies in stagnation.
9. Budget-Driven Instead of Needs-Driven Planning
Health system budgeting cycles often incentivize “use it or lose it” behavior. IT leaders may hire to preserve funding rather than to meet true needs. In today’s environment, this practice is not just outdated—it’s irresponsible. Staffing should be based on evolving requirements and strategic alignment, not fiscal habits.
10. Confusing Size with Mission Fulfillment
Many health systems take pride in being the largest employer in the communities they serve, seeing it as a badge of honor and a reflection of their community commitment. But when this identity clouds decision-making, it can lead to inflated staffing models that are misaligned with financial realities and operational efficiency. Employing a large workforce should be a means of achieving the mission—not mistaken for the mission itself. As Jim Collins reminds us: great organizations discipline themselves not around scale, but around purpose and performance. Mission fulfillment requires purposeful staffing, not symbolic scale.
Conclusion: A Call for Clarity and Courage in Health IT Leadership
Health system IT leaders stand at a crossroads. With increasing demand for digital maturity, mounting financial pressure, and a workforce in flux, the stakes for staffing effectively have never been higher. To meet this moment, leaders must confront their blind spots, let go of outdated models, and resource their teams based on facts, not feelings. It’s time to replace intuition with inspection, legacy with leverage, and complexity with clarity. That shift won’t just improve IT performance—it will amplify the mission it serves.